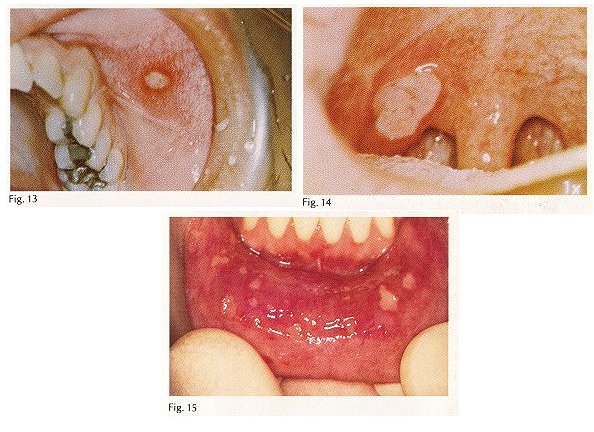
Description: This is one of the most common oral diseases. The exact incidence is unknown but estimates range from 20% to 60% of the population. lesions appear as painful ulcers ranging in size from less than 1 mm to 2 centimeters. They may be single or multiple. Small lesions (less than 0.5 cm) have been referred to as minor aphthae (Fig. 13) and large lesions (more than 0.5 cm) have been called major aphthae (Fig. 14). Major aphthae are also known as Sutton's disease. An uncommon variety of this disease appears as multiple, pinpoint areas of ulceration that seldom exceed 1 mm (Fig. 15).
Each lesion begins as a red macule, less often a papule but not as a blister. It soon ulcerates and the ulcer becomes covered by a pyogenic membrane producing the characteristic yellow-white center with surrounding erythematous flare. The shape is usually round to oval but may be elongated in natural folds such as the vestibule.
Aphthous stomatitis occurs on freely movable mucosa which does not overlie bone. The lips, cheeks, vestibule, soft palate, floor of mouth, ventral and lateral tongue are often involved but gingiva, hard palate and dorsal tongue are seldom affected.
Aphthous lesions affect all age groups from young to old but young adults, especially women, are more affected. Elapsed time between recurrences is extremely variable; some unfortunate patients have almost continuous disease whereas others go from months to years between episodes.
Etiology: The cause is unknown. The concept that canker sores are caused by an L form of Streptococcus sanguis has been superceded by theories revolving around an immunopathogenesis. The deposition of antibodies and complement within epithelium and basement membrane during the early stages of the disease suggests a humoral immune response and the influx of lymphocytes rather than neutrophils in early lesions points to a cellular immune reaction as well. It is yet to be learned if the immune response is directed against self (autoimmunity) or against an extrinsic antigen such as bacteria or viruses. To further cloud the issue, a variety of other factors have been implicated. Withdrawal of certain foods such as cheese, tomato products and gluten has been claimed to help some patients whereas in others, correction of iron, B12 and folate deficiencies have brought about a cure. Improvement of aphthous lesions during the last stages of pregnancy with exacerbation after delivery suggests that gonadal hormones may play a role. The appearance of canker sores which appear during menstruation also suggest a hormonal basis. To add a final element of mystery, aphthous stomatitis has been reported to worsen when cigarette smoking is discontinued.
There are too many theories for them all to be correct. Aphthous lesions, like cancer, may not be a single disease with a single cause but instead, a variety of diseases all manifest by painful mouth sores.
Treatment: Patients with few lesions are treated with topical analgesics or antiinflammatory agents such as Orabase with Benzocaine, Orabase Oral Paste or triamcinolone acetonide dental paste USP 0.1%.
For stronger anti-inflammatory action, fluocinonide ointment is recommended. For severe disease, favorable results have been reported using dexamethasone elixir mouthwash combined with azathioprine tablets 50 mg. bid and ibuprofen 600 mg. qid. A word of caution: azathioprine is a powerful immunosuppressant and should not be prescribed by those not experienced in its use. Prednisone is a safer immune suppressing drug. For moderate to severe disease 20 mg. daily for 7-10 days is commonly used. Patients should be cautioned about adverse effects of steroid therapy including osteoporosis, aseptic necrosis of the femoral head, cataracts, fluid retention, depression, increased appetite and exacerbation of diabetes. There is little risk of inducing the Cushingoid syndrome in short term therapy.
Prognosis: Cure is seldom achieved but palliation and long term remission may be achieved by above mentioned treatment. Without treatment, healing time varies from 4 days for a small lesion to a month or more for major aphthae. Major aphthae may also cause scarring.
Differential diagnosis: Aphthous stomatitis must be differentiated from herpetic stomatitis, the disease with which it is most often confused. Recurrence is a feature that helps to differentiate aphthous stomatitis from intraoral herpes infections. Intraoral recurrences from herpes virus infections are uncommon. Lesions indistinguishable from aphthous stomatitis have been reported in Behcet's syndrome, Reiter's syndrome, Crohn's disease and celiac disease. |