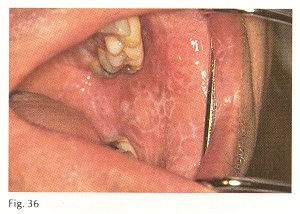
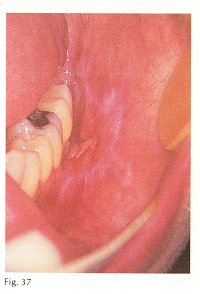
Description: Mucosal lesions of this disease appear in three forms: reticular, erosive and plaque. In the reticular type (Fig. 36) a pattern of lacy, white lines is characteristic. In the erosive type, the same reticular pattern is seen but there are areas of ulceration (Fig. 37). This is the most common form of lichen planus. In the plaque type, the lacy pattern is lost and the lesion appears as a solid white lesion. Rarely, vesicles will form. Skin is more frequently affected than is mucosa. Early skin lesions appear as red, maculopapular pruritic areas a few millimeters in diameter Oral lesions may occur on any surface but the buccal mucosa is the most common site.
Etiology: The cause is unknown but a hypersensitivity reaction is suspected. Recent reports discount the role of stress. The role of mercury is unclear but there are accounts of lichen planus-like lesions adjacent to amalgam restorations that heal when the fillings are replaced with non-mercury containing restorations. There are also reports of composite filling materials producing a similar effect. Stomatitis caused by drugs may resemble lichen planus; thiazide diuretics are chief offenders.
Treatment: The reticular and plaque types of the disease are ordinarily asymptomatic and require no treatment. In the erosive or ulcerative variety, relief is achieved with topical steroids. If ulceration is too widespread to control with topical treatment, systemic prednisone is indicated. Topical tretinoin 0.1%, a metabolite of vitamin A has been reported to be beneficial as have rinses with cyclosporin A.
Prognosis: The outlook is variable. The disease may last for years, few patients experience spontaneous remission. Topical steroids and vitamin A analogs provide relief but not a cure. Systemic steroids are effective but there are side effects and the disease may recur following discontinuance of therapy. There are reports that lichen planus predisposes the patient to oral cancer. The risk is placed at approximately 1%. The premalignant nature of lichen planus is not universally accepted. Some authors cite evidence that examples of lichen planus turning into cancer were originally dysplastic lesions masquerading as lichen planus. Such lesions have been referred to as lichenoid dysplasia. Until the dispute is settled, it is prudent to advise patients to have regular oral examinations for as long as they have the disease. Some clinicians recommend a biopsy of all patients with lichen planus.
Differential diagnosis: Lupus erythematosus, benign mucous membrane pemphigoid, leukoplakia (keratosis), erythroplasia, candidosis and lichenoid drug eruptions. |